The Five Issues
The five single-payer ‘issues’ of the Single-Payer Tornado image are addressed on this page. These issues are that single-payer will bankrupt medical providers, restrict access to drugs, raise taxation, increase patient wait times, and restrict research. Although each issue is individually addressed, many of the arguments presented extend to multiple of these ‘issues’. For the sixth and largest obstacle of single-payer healthcare presented in the ‘introduction’ page, please see the ‘insurance companies’ page under the ‘issues’ tab.

Bankrupt medical providers
Healthcare relies on the relentless work ethic of doctors and any financing system must account for how doctors will be compensated for their hard work. In order to address the payment rates, an explanation of the changes that single-payer healthcare brings is necessary. Contrary to the current U.S. system, patients do not normally participate in the payment system of single-payer healthcare. In other words, patients do not receive statements detailing the costs of each interaction and few IDs are required from patients. Similarly, doctors are spared much of the paperwork. They simply file a claim to a central government office and receive compensation. However, there is one downside to this system because the reimbursement rates of doctors tend to be smaller with single-payer systems. Health insurers often use this fact to claim that millions of jobs would be lost under a single-payer healthcare system. According to scholarly researcher and doctor James C. Shaw, “despite low reimbursement, the simplicity, predictability, and prompt payment of a single-payer have merit……registration time is minimal and billing effort is 15 to 20 hours weekly for the whole clinic. Underpayment or nonpayment is a rarity”(4). While reimbursement rates are lower per patient, single-payer healthcare offers simple payments and alleviates time for doctors to see more patients. On the other hand, Dr. James C. Shaw summaries that, “in the United States it is common to receive 50% or less of what is submitted, and many insurers routinely deny or delay claims.” To clarify, the fractured system of the United States causes far greater trouble for medical providers than lower compensation. Furthermore, professor Claudia Chaufan states that “insurance companies continue to restrict access through increasingly narrower networks of “preferred” (by them!) providers”(2). As insurance companies continue to divide doctors, the struggle of filing claims will get worse. Altogether, lower reimbursement rates with more patient appointments each day is preferable to the struggle of filing claims under the current U.S. system.
Restrict access to drugs
Due to the ginormous variety of pharmaceutical drugs and the immense diversity between patients, it is impossible to claim that any system will ever cover or even provide every drug. However, single-payer healthcare does a better job at the accessibility of medications than health insurers. Over the last several years, Dr. Mark Fendrick states that “increases in copayments have restricted access to medications, causing undesired effects, particularly among poor and elderly populations. Despite these concerns, further copay increases are expected”(5). In other words, health insurers struggle to keep the costs of drugs low which impacts accessibility. Conversely, Dr. James C. Shaw reports from Canada that, “Most employer plans cover all prescription medications with no copayment. For patients (>65 years) receiving Medicare,….noncovered drugs can be obtained for patients through applications for limited or special use”. (4) While this system is not perfect, at least senior citizens can acquire special drugs for a period of time without bankruptcy. In essence, health insurers lock away drugs behind paywalls, while single-payer healthcare removes copays and allows some access to advanced medications.

Raise taxation
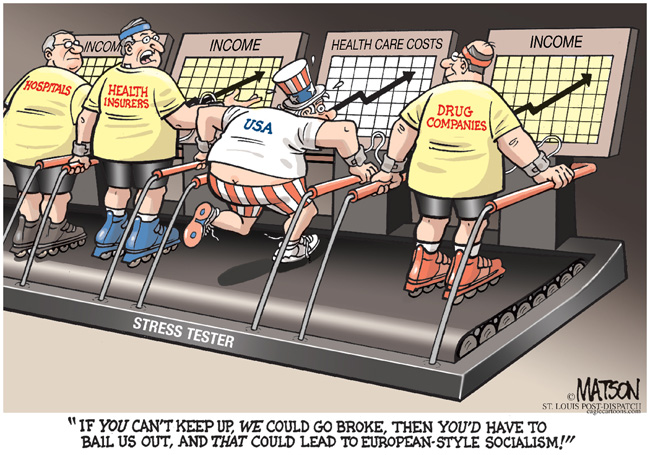
Compared to the other ‘issues’ discussed on this website, the association of single-payer healthcare with raising taxes is shocking. In reality, cost control is where single-payer healthcare truly excels. Researchers, like professor Sherry Glied, consistently state that single-payer systems, “do achieve some administrative cost savings compared to more fragmented systems”(3). These reductions originate from the power to negotiate large deals with medical suppliers as a unified system. Also, reduced paperwork and advertising save a considerable amount. After the implementation of the Affordable Care Act, health insurance stocks outperformed the S&P 500 by a stunning 106 percent. On the other hand, single-payer healthcare will control the profitability of health insurance companies and redirect excess profits into research. On top of that, numerous scholarly sources report that health insurers received a “total taxpayer bailout…[that] well exceeded $1 billion“(1). By accepting tax money, health insurance companies perform the very same deed that they accused single-payer healthcare of. At least, single-payer healthcare will spare individuals from paying premiums. These sources are addressed in-depth on the ‘insurance companies’ page under the ‘issues’ tab. After consulting her data, Professor Claudia Chaufan concludes that “the argument that “we” the people cannot afford a single-payer system is simply false—we are already paying for universal and comprehensive health care coverage, yet not getting it”(2). In other words, not only will single-payer healthcare have no effect on taxation, but it will also save expenses simply by acting as a unified system.
Increase patient wait times
When people are sick or in pain, they dread cramming into a waiting room for hours only to receive several minutes of medical attention. In the United States, health insurers fruitlessly seek to reduce patient wait times and many wonder how single-payer healthcare will handle this issue. When Dr. James C. Shaw compared the Canadian and American healthcare systems in his scholarly article published in The American Journal of Medicine, he specifically mentioned that registration/billing times in Canada took around 15 to 20 hours weekly for the whole clinic of six doctors. Meanwhile, a clinic of two doctors in the United States needs at least one full-time employee dedicated solely to registration/billing (4). After two hundred hours worth of shadowing experience, I can personally affirm that doctors spend more time on paperwork than they do on patients in the United States. When single-payer healthcare is implemented, the straightforward system will enable doctors to focus on patients. As the productivity of doctors rises, patient wait times will decrease. Hypothetically, patient satisfaction will rise even if patient wait times do not improve. This is due to the simple nature of single-payer healthcare. Patients will no longer have to cope with employers constantly changing their health plans and they will no longer have to choose between the ever-narrowing list of ‘approved’ providers. Overall, Single-payer healthcare will reduce patient wait times by taking away the unnecessary distractions stealing the attention of doctors from patients and the direct rules of single-payer healthcare will boost patient satisfaction.
Restrict research
The Single-Payer Tornado image protests against the horrors that single-payer will inflict on America’s medical research system, however, there’s little connection between single-payer healthcare and medical research. As Professor Deborah Stone points out, “single-payer is a simple idea about consolidating payment, with nothing to say about who will set the criteria for deciding what services are covered, let alone which services are highly and not so highly valued”(6). To clarify, single-payer healthcare is simply a financing system and it is up to the policymakers to decide where the money goes. Therefore, the decrease in research may be the result of a decision to invest more healthcare provided to the people. Furthermore, the statement made by The Single-Payer Tornado image is very suggestive. To put it differently, if single-payer healthcare reduces the number of drugs invented yearly for a hundred to ninety-six then that is barely a loss. On top of that, a new drug can have no impact on healthcare due to a variety of reasons. For instance, it could be expensive to manufacture or the new drug could treat a minor condition that was already treatable. Given these points, single-payer healthcare will not necessarily impact medical research because research money is determined by policymakers and the size of the supposed impact is disputable.
Conclusion:
As a whole, The Single-Payer Tornado image summarizes five common misconceptions concerning single-payer healthcare. The aforementioned arguments aimed to disperse these myths and provide a glimpse of the complex nature of healthcare. Overall, single-payer healthcare outperforms the current American health insurance system in every aspect. Nevertheless, single-payer healthcare is not flawless and the performance of the system relies on its implementation by policymakers. Since other countries successfully enacted this system there is no doubt that the United States could do so also.

Footnotes:
1.“House Hearing, 113th Congress – POISED TO PROFIT: HOW OBAMACARE HELPS INSURANCE COMPANIES EVEN IF IT FAILS PATIENTS.” Govinfo, 18 June 2014, www.govinfo.gov/app/details/CHRG-113hhrg88826/CHRG-113hhrg88826/summary.
2.Chaufan, Claudia. (2015). WHY DO AMERICANS STILL NEED SINGLE-PAYER HEALTH CARE AFTER MAJOR HEALTH REFORM?. International journal of health services: planning, administration, evaluation. 45. 149-60. 10.2190/HS.45.1.l.
3.Glied, and Sherry. “Single Payer as a Financing Mechanism.” Journal of Health Politics, Policy and Law. Duke University Press, August 1, 2009. https://read.dukeupress.edu/jhppl/article/34/4/593/93606/Single-Payer-as-a-Financing-Mechanism.
4. Shaw, James C. “Oh, Canada: Comparing Single-Payer Health Care with Practice in the United States.” The American Journal of Medicine 118, no. 10 (2005): 1064–66. https://doi.org/10.1016/j.amjmed.2005.05.017.
5.Fendrick, Mark, and Dean G. Smith. “A Benefit-Based Copay for Prescription Drugs: Patient Contribution Based on Total Benefits, Not Drug Acquisition Cost.” The American Journal of Managed Care 7, no. (9) (October 2001): 861–67. https://www.researchgate.net/publication/11778261_A_Benefit-Based_Copay_for_Prescription_Drugs_Patient_Contribution_Based_on_Total_Benefits_Not_Drug_Acquisition_Cost.
6.Stone, Deborah. “Single Payer—Good Metaphor, Bad Politics.” Journal of Health Politics, Policy and Law 34, no. 4 (2009): 531–42. https://doi.org/10.1215/03616878-2009-014.